
Along with GDP, education level/literacy rate, and life-expectancy, assessing how well a nation is able to provide its citizens with access to health care can be very informative. Health care systems are made up of patients utilizing the system, health care providers, and resource suppliers whether that be insurance companies or medical equipment manufacturers. Observing how well these key stakeholders interact allows us to assess the health care system’s effectiveness. Health care systems SHOULD evolve over time, as culture/society, our understanding of diseases, and our technological capabilities grow. Health care can be expensive, but should not be a luxury only wealthy people can enjoy. As stated in Mills (2014), improving a nations health care system is a long-term goal.
The United States’ world rankings in health care have steadily declined across the past few decades. This places the US firmly behind a number of low- and middle-income countries and firmly behind almost all high-income countries, as the US faces many of the issues mitigated by other nations.
![]()
[Source: The Commonwealth Fund 2016]
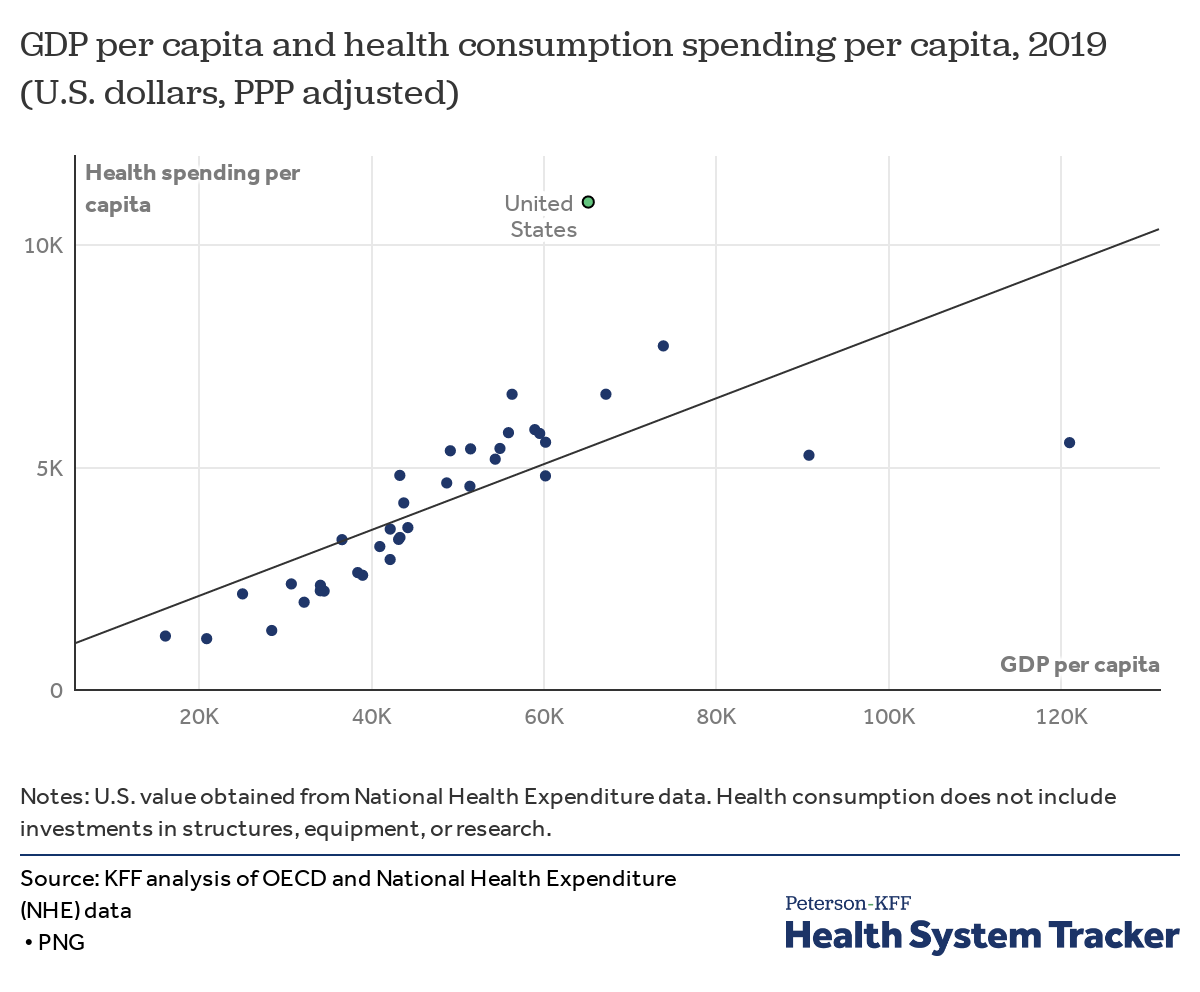
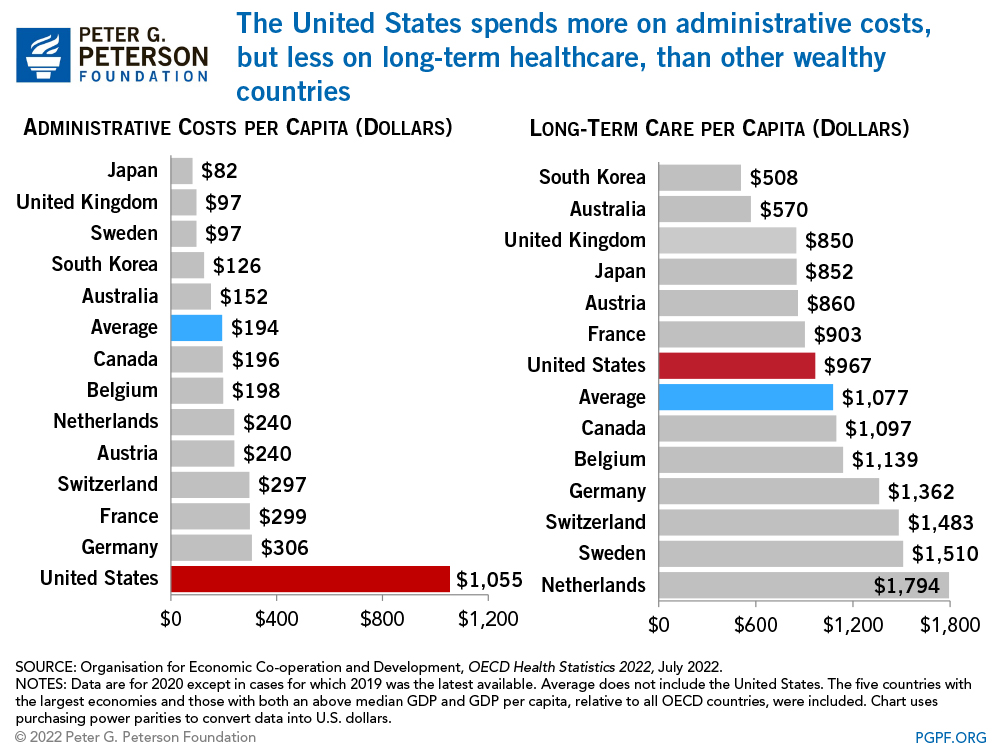
While the US ranks relatively low in health care quality, access efficiency and equity it ranks disproportionately high in health care spending. We are well above the average for comparable countries. And while the United States spends more on health care, health outcomes are not generally better than other nations as we lag behind in life expectancy at birth, infant mortality, and other general metrics assessing health status. Western nations with comparable GDP like Germany, Switzerland, and Scandinavian nations are spending a fraction of what the US does, while maintaining better results.
 With out-of-pocket payments making up a significant chunk of health care financing in low- and middle-income countries, identifying creative ways to cover the cost is imperative. According to a 2016 Kaiser Family and New York Times survey, more than 25% of Americans had trouble paying a recent medical bill.
With out-of-pocket payments making up a significant chunk of health care financing in low- and middle-income countries, identifying creative ways to cover the cost is imperative. According to a 2016 Kaiser Family and New York Times survey, more than 25% of Americans had trouble paying a recent medical bill.
We are one of the last high-income/developed nations to resist universal healthcare. Universal health care would mean ejecting on our current single-payer model of health insurance coverage and more readily adopting social health insurance. Spreading the risk of health care causes across a large population of people should be a no-brainer for Americans, and yet… there is unyielding resistance from some political groups.
The current US health system is a mix of both private and public insurers and health care providers. Former President Barack Obama, against gnash republican obstruction, was able to enact the Affordable Care Act in 2010 to expand coverage, slow health care spending, and improve clinical quality. Sadly, the ACA was somewhat neutered by the following administration, which was known throughout its short tenure for many overtly racist communications and policies. The ACA was a small step in the right direction, but still not quite the universal health care goal we should be striving for.
Mill (2014) points out that there is no single way to develop a health care system that will work for all nations and stakeholders, but we do have multiple working blueprints for success. One characteristic highlighted is to “take into account the constraints imposed by history and previous decisions”. This, to me, is a clear opportunity for policy makers to address and rectify historically perpetuated inequities by the US government. Not only has access to equitable care been withheld from many communities, but toxic health practices in studies of Black communities has tarnished the relationship between minority [would be] subjects and researchers. Repairing this relationship is vital to achieving health equity.
The Civil Rights Movements provided incredible advancements for minorities to gain access to quality health care and reducing segregation in American medical institutions. In some instances, communities went from literally nothing to something through clinics set up with volunteer physicians. but health disparities continue to ravage minority and impoverished American communities.
As stated in Napier et al (2014), understanding how culture plays into health outcomes is a vital key to reducing health inequity, not only in the United States, but in low- and middle-income countries as well. Napier describes the overlap of cultural competence, health inequities and community of care and how health and wellbeing are fundamentally tied to cultural perceptions. Without pointing blame at past wrongs, interventions that engage community stakeholders with the other layers of health care systems should be prioritized. As we’ve mentioned cultural differences within the country, its important to recognize that the developed nations we’ve compared the US to are also fundamentally culturally different, thus their specific fixes might not fit here.
The road to meaningful health care reform is an uphill one, for both the US and developing nations, but progress is continuously being made. There are some positives to the US health care system, including quality of health care services, minimal waiting lists for major procedures and adequate resources. However, the negatives of expensiveness, limited insurance coverage and minimal to no preventive care presently outweighs to good. Overall, the lack of access to care for all casts a harrowing shadow over America’s health future. We’ve seen how our nation has responded to a global pandemic… If we do not learn some needed lessons, I can’t imagine how things will look after the next inevitable public health crisis.

Awesome blog! It still baffles my mind that the US is one of the last developed nations to resist universal healthcare. If the US health system could even adopt some things from universal healthcare the health and lives of American’s would improve greatly!
I agree the statement on the ACA being a right step in the right direction. There are multiple steps that can be taken to begin developing a better health care system, one being to understand the health disparities across the United States. Atlanta is a clear cut example of these disparities in health due to racial and cultural differences, and could be addressed to improve the communities access to health services. The lack of access to health care in the US is frightening, and I truly hope we learn from this global pandemic.