
Health Disparity: “a particular type of health difference that is closely linked with social, economic, and/or environmental disadvantage.”
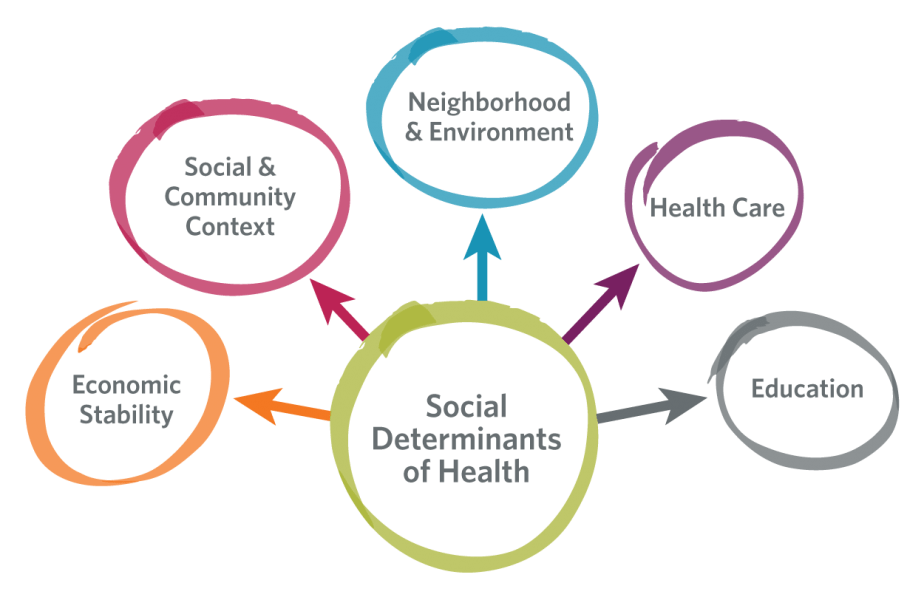
Powerful, complex relationships exist between health and biology, genetics, and individual behavior, and between health and health services, socioeconomic status, the physical environment, discrimination, racism, literacy levels, and legislative policies. These factors, which influence an individual’s or population’s health, are known as determinants of health.
Kim Anderson is a successful Atlanta executive and lawyer. She is African American and graduated from Columbia Law School in 1984. Ms. Anderson enjoys high socio-economic status, eats well, exercises regularly, and has never smoked. She has all the social determinants in her favor, and still she gave birth to a premature baby.
So, what did it go wrong?
According to Kaiser Family Foundation: “Black and American Indian or Alaska Native (AIAN) individuals continue to fare worse compared to White individuals across most examined measures of health status, including physical and mental health status; birth risks; infant mortality rates; HIV and AIDS diagnosis and death rates.”
Infant mortality among White American women with a college degree is about 4 deaths per 1,000 live births, but among African American women with the same level of education, infant mortality is 10 deaths per 1,000 live births. In addition to child mortality rates, African American women experience disparities in maternal mortality, which is three times higher than the mortality of white American mothers.
Does genetics explain the differences?
When all the other factors are the same, maybe it is just a matter of genetics. Well, research says this is not the case. Genetic differences do not explain health disparities, and furthermore, there are more genetic differences within race than between races. So race is not a biological construct which reflects health disparity differences, it is a social construct.
All the race-associated differences related to health care access and health care outcomes are in fact due to the effect of racism.
Racism is not just about discrimination and prejudice. Dr. Jones explains racism on three levels; institutionalized, personally mediated, and internalized.
Institutionalized racism is defined as differences in access to the goods, services, and opportunities of society by race. It includes differential access to education, employment, medical care and information.
Mediated racism is about prejudice which is differential assumptions about the abilities and motives of others according to their race, and discrimination which is differential actions towards others according to their race.
Internalized racism is when members of the stigmatized races accept the negative messages towards them. It means accepting the not-true “limitations” and also not believing others who look like them. Internalized racism is what black medical doctors face from black patients, which are usually sceptical towards their doctor’s abilities.
How is racism manifesting itself in other health related conditions:

Well, health disparities related to race and ethnicity are widespread in different health conditions. According to CDC: a higher percentage of black women (37.9%) than white women (19.4%) died before age 75 as a result of CHD, as did black men (61.5%) compared with white men (41.5%).
Black females have a higher obesity prevalence.
One of every five infants born to non-Hispanic black mothers in 2007 was born preterm, compared with one of every eight to nine infants born to non-Hispanic white and Hispanic women.
The rate of preventable hospitalizations is higher among non-Hispanic blacks.

Current asthma prevalence is higher among the multiracial, Puerto Rican Hispanics and non-Hispanic blacks than among non-Hispanic whites.
Black teens and adults have an over eight times higher HIV diagnosis rate.
And lastly, COVID -19 brought all the disparities to the surface. Racial and ethnic minorities are being disproportionately affected by COVID-19. Black or African American are 4.7 times higher to be hospitalized and 2.1 times higher to die from COVID-19.
Ms. Anderson’s baby survived, but health disparities faced by people of different race and ethnicity “are symptoms of broader underlying social and economic inequities that reflect structural and systemic barriers and biases across sector.”
So, what is being done to address the issues?
First of all, is important to say that recognizing and understanding health disparities is the first step to better address them.
And we are becoming more sensitive to the issue. Let’s take for example the Black Lives Matter Movement, which is a social movement emphasizing basic human rights and racial equality for black people. The protests to support the movement spread quickly in over 2,000 cities and towns in over 60 countries. There are estimations that between 15 million and 26 million participated at some point in the demonstration.

The CDC is also accelerating its efforts to eliminate health disparities with a focus on surveillance, analysis and reporting of disparities.
Some of the actions that they are taking are:
- Increase community awareness of disparities as problems with solutions
- Set priorities among disparities to be addressed at the federal, state, tribal, and local levels
- Articulate valid reasons to expend resources to reduce and ultimately eliminate priority disparities
- Implement the dual strategy of universal and targeted intervention strategies based on lessons learned from successes in reducing certain disparities (e.g., the virtual elimination of disparities in certain vaccination rates among children)
- Aim to achieve a faster rate of improvement among vulnerable groups by allocating resources in proportion to need and a commitment to closing gaps in health, longevity, and quality of life
And lastly, what does it mean on a global level ?
Health disparities are not just within the country, they are also among the countries. According to WHO, children in the sub-Saharan Africa are 14 times more likely to die before the age of five than children in other parts of the world. Developing countries account for 99% of maternal deaths in the world and around 95% of tuberculosis deaths come from developing countries.
Health inequalities slow development and are a huge burden to the economic, costing each year around 1.4% of gross domestic product.
In times like these, the BLM Movement gives hope that people are becoming more aware that racism is beyond what we knew.

There are no comments yet...Kick things off by filling out the form below.